
Corona virus–The story of Heist, Storm and The Surgical Strike
New Delhi : By this time all of us are well aware of what the Coronavirus is, the COVID19 pandemic and the appropriate precautions to safeguard against the infection. However, the complex pathways in which the virus affect the human body is a work in progress, everyday new case studies come revealing more about the nature of the virus and the human immune response to it. Studies show that the overzealous immune system might be as dangerous as the virus itself. In this article we take you through the intricate route the virus takes in our bodies and how the body defends itself.
The Coronavirus
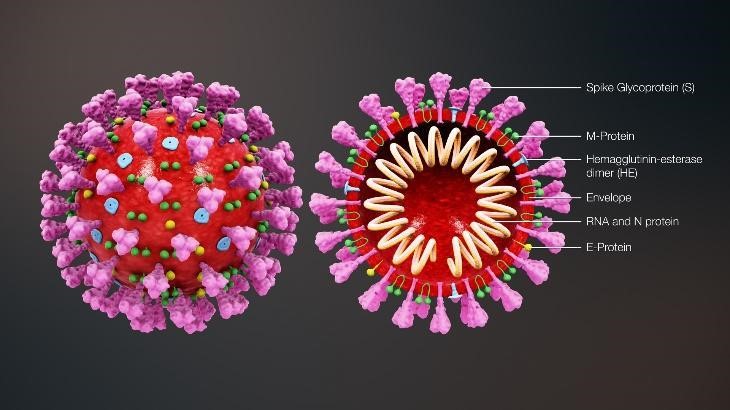
Let’s have a look at the structure of the SARSCOV2 which is relevant to this article. This is a drawing of the Novel coronavirus. On the surface, you can see surface projections akin to the image of a crown or the solar corona, hence the name- CoronaVirus. These projections are proteins each handling a specific function for the virus. Two of those proteins are of interest here: the Spike protein, and the HE protein.
On the inside we can see the genetic material of the virus- The single stranded RNA which contains the information for the virus to make a copy of itself. The primary modes by which the Coronavirus gets transmitted is by respiratory droplets and fomites. New studies suggest that SARSCOV2 can spread aerosolized and through fecal-oral routes. Once inside the body the virus can infect multiple different cells in multiple tissues in the body.
The Heist
The virus enters the body through nose, mouth or other mucous membranes on the face, that’s the reason why it is repeatedly being told not to touch your face often. Virus is basically an inert material outside the body, it does not have any capabilities for its own reproduction, and technically the virus is not alive. But once inside the body, that’s a different ball game altogether.
Once the virus is inside, it needs the help of a cell to reproduce itself, but the cells do not allow the entry of foreigners inside their premises. Thus the virus needs to sneak in like a thief, clandestinely.
The virus predominantly infects the lungs. Cells in our body have different kinds of receptors, each having a definite purpose, like communication with neurotransmitters, hormones, transport of nutrients etc. Receptors can be considered as doors, which can be opened only by a specific key. The corona virus uses the Spike Protein and the HE protein, like a forged key, to open up a particular type of receptor on the cell, called the Angiotensin Converting Enzyme -2(ACE 2) receptor, whose original function is blood pressure regulation, among others. Assisting in this unauthorised intrusion is the Transmembrane Serine Protease 2 (TMPRSS2), a known human airway enzyme.
The Corona virus uses S Protein, HE protein as the forged key with the help of TMPRSS2 to bind into the ACE2 receptor. Once bound, the cell itself will take the virus inside by a mechanism known as endocytosis. Researchers have used Cryogenic Electron microscopy to demonstrate this mechanism. Once inside the cell, the virus releases its genetic material- The RNA inside the cell.
The cell is a very complicated machinery having many organelles, each serving a role. Here in the cell we have a machine called ribosome whose purpose is to encode proteins needed for the human body as dictated by the nucleus in the cell. The nucleus communicates with the ribosome via an RNA called the messenger-RNA(mRNA), now RNA of the virus masquerades as the mRNA and tricks the ribosome by giving it the recipe to make parts of virus instead of proteins needed for the human body.
These viral proteins are called polyproteins i.e. the components which are needed to make the S-Protein, HE protein etc. In addition to this, the viral RNA uses the help of an enzyme called the RNA-dependent RNA Polymerase(RdRP); this enzyme is super cool as it catalyses the viral RNA to make more viral RNAs! These RNAs will in turn make more polyproteins and this vicious viral cycle continues.
These proteins and RNA move into the endoplasmic reticulum–Golgi intermediate compartment (ERGIC) which facilitates the sorting of these cargo, further into the Golgi body where all the components of the virus are packaged into a vesicle. A New virus is born.
Swindling up all the resources of the cell, and leaving it to die, the virus exits the cell via a process called Exocytosis. The Heist is complete.
The Storm
The Lungs can be imagined like an inverted tree with a trunk, branches and leaves. The leaves are the ‘Alveoli’, through which oxygen is absorbed and carbon dioxide is excreted.
The ACE2 receptors where the S-protein attaches are found throughout the body like but mainly in the Type 2 Pneumocytes in the lungs. Type-2 Pneumocytes are cells in the alveoli that produce surfactants- the compounds essential for life as it lines the alveoli to lower surface tension, thereby preventing the collapse of the lung during expiration.
Once the virus infects these cells, the cells start dying, but not before sending a distress signal via compounds called interferons. Cells send signals to nearby healthy alveolar cells that there’s a virus in the vicinity and urge them to start increasing the synthesis of antiviral peptides. These peptides can potentially break down the virus or prevent attachment of the spike proteins. Whenever these cells are damaged, they also start to release compounds called pathogen-associated molecular patterns (PAMPs) and danger-associated molecular patterns (DAMPs). In addition to this, the cells also start releasing inflammatory chemicals called cytokines. In essence, the cells broadcast that they are under attack. This call for help activates the first responders, the guards of our Immune system – the Alveolar macrophages. The macrophages in the vicinity now rush up to look at what’s wrong, turning the site of infection into a battlefield.
Macrophages eliminate viruses by literally devouring them, while simultaneously signalling other cells via inflammatory cytokines. One of the outcomes of this cytokine signalling is that the capillaries (tiny blood vessels) outside the Type 2 pneumocytes starts releasing fluids to the space between the alveoli and the capillary, this is called the interstitial oedema, just like your finger swells when there is a cut or a bruise. In the finger, this oedema is helpful in fighting the infection, but not in the lungs; it is through the thin wall between the alveoli and the capillary that the gas exchange takes place, i.e. absorption of oxygen from the lungs and releasing the carbon dioxide, once fluid accumulates in this area the concentration of oxygen in the blood drops. This condition is called hypoxemia, the patient experiences shortness of breath. Meanwhile, the macrophage calls in for heavy back up by further cytokine signalling. Neutrophils now leave their patrol route in the bloodstream and move to the site of infection, along with more macrophages. This is called the innate immune system. Once the neutrophils arrive, all hell breaks loose.
The Neutrophils start secreting particular types of molecules called Reactive oxygen species as well as proteases . These molecules try to destroy whatever is causing the inflammation. Neutrophils are so lethal that along with viruses they also damage healthy lung cells. Neutrophils’ protective effect during antiviral defence has been controversial, because they have been reported to mediate both beneficial and detrimental effects to the host. In the process of attacking the virus neutrophils damage the surrounding healthy cells i.e. Type 1 and Type 2 Pneumocytes ; we already learned that the Type 2 Pneumocytes makes surfactants, and the Type 1 Pneumocytes is where the gas exchange takes place, i.e. the breathing process. The damage received by the Type 2 Pneumocytes causes decreased surfactant production and tends the alveoli to collapse, further exacerbating already worse low oxygen in the blood. Collateral damage to Type 1 Pneumocytes again causes low blood oxygen, and the patient now gasps for breath and now probably moved to the Intensive care unit.
The alveoli are damaged not only by the virus but also by the Reactive oxygen species and the proteases released by the neutrophils. More damaged cells cause more signalling for help and a vicious cycle emerges, this is called the cytokine storm. It is not fair to blame neutrophils alone for the carpet bombing like activity, others like dendritic cells and macrophages also join the party which we will discuss in the coming paras. This cytokine storm signals to the central nervous system to increase the body temperature, stimulate cough reflux, the cytokines also promote coagulant activity and decrease anticoagulant activity in the blood, in very severe cases a clot can be formed and is potentially fatal.
This uncontained cytokine signalling can lead to pneumonia and potentially to Acute Respiratory Distress Syndrome (ARDS) and further to Systemic inflammatory response syndrome – an inflammatory state affecting the whole body, creating a perfect storm. New research shows that in addition to the attack on the lungs SARSCOV2 directly attacks the heart, lungs, intestines, kidneys, potentially wherever the gateway of ACE2 exists. Both these conditions, along with coinfections, may lead to multiorgan failure, the patient is now probably on a ventilator. COVID-19 virtually turns your Immune system against you, meanwhile, the Cytokine Storm continues.
The Surgical Strike
While the first line of defence, the neutrophils and the macrophages are busy fighting the virus, the Intelligence wing of the immune system kicks in- the Dendritic celḷ. The dendritic cells belong to a class of cells called ‘Professional Antigen presenting cells’. Remember the PAMPS and DAMPs we discussed earlier, those along with the parallel cytokine storm activates the dendritic cell. The dendritic cells inspect the site of the battlefield and samples the part of the virus(antigen) and displays in its outer surface, akin to a tribal lord wearing the bones of his slain enemy, through a protein called the Major Histocompatibility complex 2(MHC2), hence the name Antigen presenting cells. The Dendritic cells then travel to the Armed forces headquarters- i.e. the Lymph nodes, where millions of the elite commando force – T cells, are waiting to be activated, thus initiating the adaptive immune response. Dendritic cells are critical because they act as the bridge between the innate and the adaptive immune response.
The T cell is unique as it has a T-cell receptor (TCR) on the surface that is responsible for recognizing fragments of antigen bound to MHC2 of the dendritic cells. Once the T cell identifies an antigen submitted to it by the dendritic cells, a chain reaction starts, the T cells begin to replicate itself into Helper T cells, Natural Killer(NK) cells, Memory cells and Regulatory cells.
The NK cells are the contract killers of the immune system who have undergone an assassin training programme in the thymus gland. They move to the battle field, identify infected cells and destroy them via a process called apoptosis, if they are beyond repair.
Helper T cells are arguably the most important cells in adaptive immunity. The Helper T cells not only signal the macrophages to be aggressive in killing and to destroy the ingested virus, but also help activate Natural Killer cells to kill the infected cells. The Helper T cells move to the centre of the lymph node to activate a powerful weapons factory- The B cells.
Like the T cells, the B cells also have unique receptors called B-Cell receptors (BCR), – ‘Y’ shaped molecules on the surface of the B-Cell. The tips of the Y is a variable region and the long arm is a constant region. By variable region it is meant that each tip of the “Y” contains proteins specific for one particular type antigen, allowing the antigen and the Y tip to bind together with precision.
The helper T cells now having reached the centre of the lymph node carrying the antigen in its MHC2, needs to find a complementary binding site in the BCR which is akin to a jigsaw puzzle. An antigen is a foreign body which can come in millions of varieties, the T cells begin an arduous search for an exact match to complete the jigsaw puzzle. Rest assured that there will be at least a few B cells which are having the perfect match, as evolution has endowed us with this ability. Once the T cell finds the exact B cell, a cascading reaction starts, the type of B cells which have this particular setup of BCR to complete the jigsaw begins to proliferate to immunoglobulin-secreting cells known as Plasma B cells
Plasma B cells produce precision heat seeking missiles – the immunoglobulins popularly known as antibodies, which are closely modelled like that of the B cell receptors. Figure 2 gives a better understanding. The Surgical Strike Begins.
B Cells themselves are Antigen presenting Cells, they also display the antigen specimen in their MHC2, communicating to more Helper T cells and thus to more B-Cells. This chain reaction continues and a huge inventory of antibodies are produced. These antibodies are known by various names as IgM, IgG etc. Armed to the teeth, millions of antibodies move to the battlefield, giving macrophages the much-needed air support. The antibodies bind to the virus as in a lock and key mechanism, each antibody is so unique to the antigen that they bind only to the virus and not to any other healthy cells. Once bound they become what is known as an ‘immune complex’, or an ‘antigen-antibody’ complex, which are like sitting ducks to be devoured by the other cells of the immune system. Now the balance shifts, in a team effort the virus is obliterated, the patient is now slowly moved out of the ICU and can breathe fresh air. Once the infection is cleared the immune cells which are no longer needed does Harakiri and are self-destructed. Memory T cells and Memory B cells stay back, which retain the memory of the antigen and remain in the system, so that next time when the virus is encountered, they are terminated even before we notice. The Surgical Strike is complete.

SARSCOV2, unlike SARSCOV1 is dicey that it can infect the very T cells, just like HIV, which might explain its rapid infectivity, fortunately the virus is not able to replicate inside the T cell and is a dead end for the virus, but still enough for a reduced T cell count.
This is an oversimplified version of the immunological response; each cell activates the other by a series of complex chemical pathways. Antigen presentation, B cell activation etc. are always done by multiple confirmatory signalling, and we have overlooked the role of the ‘complement system’ which is integral to our Immunity.
Our immune system is a complex, elegant orchestra playing the exact tune to save your life. Life is mind bogglingly complicated but if we take the time to understand it what awaits is endless wonders and awe-inspiring beauty. If you ever feel lonely or unloved, remember that an army of tiny teeny cells are always in love with you, fighting to their death, to keep you alive. Take care of your immune system and it shall in turn take care of you.
DV Vinod Kumar
The author is an officer of the Indian Information Service.
(The contents in this article is for educational purposes only.
Views and opinion are personal to the author.
The author can be reached at [email protected])







